
There’s a huge current trend in more advanced clinics to buy a hemoanalyzer and count the platelet content of the PRP produced by the clinic. While on the surface, this would seem to be a noble effort, the devil is always in the details. Regrettably, the fine print on this one shows that most of these counts are likely more fiction than fact. Let’s dive into the science to see what’s going on.
PRP and Platelet Counts
When I founded Regenexx in 2005, we had some basic science observations from our lab that were hard to ignore. Basically, when using the patient’s platelet lysate to grow their mesenchymal stem cells in culture, in middle-aged and older patients, the higher the platelet dose, the better the growth of their stem cells. Hence, when we began using platelet-rich plasma (PRP), we knew that for most of our patients, a higher dose was better. At the time, however, the few clinics that were offering PRP were using off-the-shelf systems that could only produce low-dose PRP. Fast forward almost two decades and the current wisdom based on in-vitro studies and clinical trial results confirms that higher-dose PRP beats lower-dose PRP (2-6). As a result, we see many more advanced practices beginning to count the platelet content of their PRP.
At first blush, buying a machine to count the platelet content of your PRP seems to be a best practice sort of thing, right? It shows an additional devotion to the art that can’t be denied. Having said that, like everything else in life, the fine print or details often get in the way of the best of intentions.
Learn More About Regenexx® Procedures
Request a digital booklet and more information to learn about alternatives to orthopedic surgery and the Regenexx patient experience.
Platelet Counting 101
First, a machine that counts blood components is called a hemoanalyzer. These machines are designed specifically to count platelets in whole blood, and that little factoid will become important as we explore how they work.
A commonly used hemoanalyzer machine today is one produced by Horiba. The Micros range of products is often sold to clinics to count platelets in PRP. They use an impedance method to identify and count cells. This means that cells in an electrolyte solution are passed one by one through a small aperture surrounded by two electrodes. As they pass through, changes in voltage are recorded, indicating cell count and size.
However, impedance counters (and all automated cell counting methods for that matter) have a problem. This is from a guide to cell counting technology (1):
“Because these instruments count cells one-by-one, aggregated and complex cell types cannot be counted by these instruments.”
This problem is counting aggregates, which will become very important as we look at counting the platelet content in PRP.
Platelet Aggregates 101
Platelets are built to aggregate and cause a blood clot. While adding anticoagulants like ACD will help reduce those aggregates, the more platelets are concentrated and agitated by the process of making high-dose PRP, the more likely they are to aggregate anyway. The biggest issue for accurate platelet counts is when two or three platelets stick together (doublets or triplets). These small aggregates will now have a size and impedance more similar to a red or white blood cell than a platelet, so they get miscounted as something else. In this case, the platelet count reported by the machine goes down, while the red or white blood cell count goes up.
A Confused Doctor
One of our affiliates recently bought a Horiba hemoanalyzer because it’s the same one we use in the CSC and Regenexx labs. He was confused because his counts seemed off, and he knew that some of this was happening due to aggregates. This was the answer of Dustin Berger, one of our scientists, which contains a critical message for all physicians involved in platelet counting:
“What you describe is not uncommon. The more concentrated a PRP becomes, the greater the prevalence of platelet clumping. These clumps are subsequently read as lymphocytes by the Micros60, resulting in lower platelet counts and higher WBC counts than what is truly present.
The following plots show platelet counts from 4X, 10X, and 20X PRPs (mean +/- SD, n=10). Note at the 4X concentration that there’s ~4-fold increase in platelet concentration…however, at the 20X concentration, there’s only a ~15-fold increase. As you’ve stated, this is not due to lost platelets, but platelet clumping.
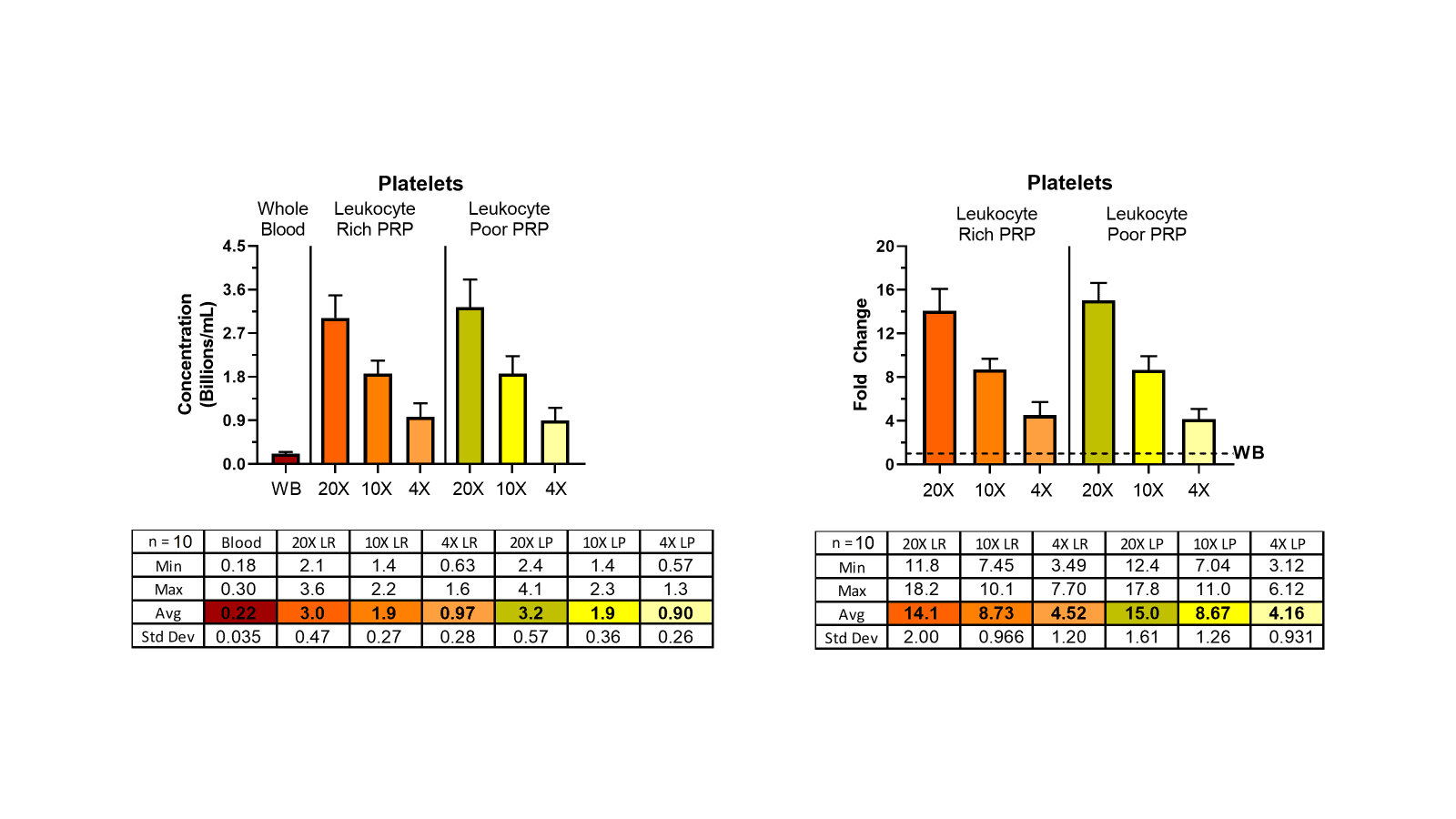
Moreover, we’ve been able to confirm clumping by adding the platelet aggregation antagonist PGI2 (prostacyclin) at 1uM and observing an increase in platelet counts with a concomitant decrease in WBC counts. However, this is not a clinical solution.
Your approach to counting seems sound. I don’t have a lot of personal experience vortexing cellular samples…I was always cautioned against it in graduate school. Though there is clearly published precedence for doing so to reduce platelet clumping prior to counting.
https://academic.oup.com/labmed/article/28/10/665/2503680
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10064346/
One thing you could do would be to count plasma prior to concentrating and PPP post concentrating to get a better picture of total number of platelets in the PRP, but that doesnt address the clumping issue.”
The Bottom Line on PRP Counting
There is no practical way to get an accurate platelet count of high-dose PRP using a hemoanalyzer. While you can help the count by performing tricks like vortexing or counting lost platelets in the platelet-poor plasma, you will always be at the mercy of a machine never designed to count PRP.
So, while I’m not against advanced practices buying hemoanalyzers and counting platelets, we all need to realize that the data produced by these efforts is flawed.
The upshot? Like anything in life, there is the simple conception of reality and then the fine print. In this case, the most advanced understanding of what happens when you put PRP into a hemoanalyzer creates significant uncertainty that buying one of these expensive machines is worth it for the average practice.
______________________________________________________________________________
References:
(1) Chemometec. The Ultimate Guide to Cell Counters in the Life Sciences. https://chemometec.com/the-ultimate-guide-to-cell-counters/ Accessed 6/20/24
(2) Berrigan WA, Bailowitz Z, Park A, Reddy A, Liu R, Lansdown D. A Higher Platelet Dose May Yield Better Clinical Outcomes for PRP in the Treatment of Knee Osteoarthritis: A Systematic Review. Arthroscopy. 2024 Mar 19:S0749-8063(24)00206-8. doi: 10.1016/j.arthro.2024.03.018. Epub ahead of print. PMID: 38513880.
(3) Patel S, Gahlaut S, Thami T, Chouhan DK, Jain A, Dhillon MS. Comparison of Conventional Dose Versus Superdose Platelet-Rich Plasma for Knee Osteoarthritis: A Prospective, Triple-Blind, Randomized Clinical Trial. Orthop J Sports Med. 2024 Feb 26;12(2):23259671241227863. doi: 10.1177/23259671241227863. PMID: 38410168; PMCID: PMC10896053.
(4) Bansal, H., Leon, J., Pont, J.L. et al. Platelet-rich plasma (PRP) in osteoarthritis (OA) knee: Correct dose critical for long term clinical efficacy. Sci Rep 11, 3971 (2021). https://doi.org/10.1038/s41598-021-83025-2
(5) Berger DR, Centeno CJ, Steinmetz NJ. Platelet lysates from aged donors promote human tenocyte proliferation and migration in a concentration-dependent manner. Bone Joint Res. 2019 Feb 2;8(1):32-40. doi: 10.1302/2046-3758.81.BJR-2018-0164.R1. PMID: 30800297; PMCID: PMC6359887.
(6) Anitua E, Sánchez M, Zalduendo MM, de la Fuente M, Prado R, Orive G, Andía I. Fibroblastic response to treatment with different preparations rich in growth factors. Cell Prolif. 2009 Apr;42(2):162-70. doi: 10.1111/j.1365-2184.2009.00583.x. Epub 2009 Feb 24. PMID: 19250293; PMCID: PMC6496288.
View Profile
If you have questions or comments about this blog post, please email us at [email protected]
NOTE: This blog post provides general information to help the reader better understand regenerative medicine, musculoskeletal health, and related subjects. All content provided in this blog, website, or any linked materials, including text, graphics, images, patient profiles, outcomes, and information, are not intended and should not be considered or used as a substitute for medical advice, diagnosis, or treatment. Please always consult with a professional and certified healthcare provider to discuss if a treatment is right for you.
- SEO Powered Content & PR Distribution. Get Amplified Today.
- PlatoData.Network Vertical Generative Ai. Empower Yourself. Access Here.
- PlatoAiStream. Web3 Intelligence. Knowledge Amplified. Access Here.
- PlatoESG. Carbon, CleanTech, Energy, Environment, Solar, Waste Management. Access Here.
- PlatoHealth. Biotech and Clinical Trials Intelligence. Access Here.
- Source: https://regenexx.com/blog/why-counting-platelets-in-high-dose-prp-can-be-a-fools-errand/