Baseline characteristics
A total of 52 adult patients with R/R DLBCL were identified and enrolled. The median age at diagnosis was 45 years (range, 17–63), with marginal male predominance (n = 30, 57.7%). 36 patients (69.2%) were identified as having an advanced-stage disease (Ann Arbor stage III–IV), whereas 15 (28.8%) suffered from B symptoms. Thirteen patients (25.0%) had BM involvement of DLBCL at the time of diagnosis, and 8 of 13 (61.5%) had complex karyotypes. All enrolled patients were classified as low (n = 15, 28.8%), low-intermediate (n = 13, 25.0%), high-intermediate (n = 14, 26.9%), and high (n = 10, 19.2%) risks based on international prognostic index (IPI) risk classification. Four patients had a double-hit mutation (7.7%), and according to Han’s criteria, 32 and 13 patients were categorized as ABC type (61.5%) and GCB type (25.0%), respectively. The baseline characteristics at the time of diagnosis are summarized in Table 1.
Allo-HSCT characteristics
Notably, most enrolled patients had previously undergone intensive treatments, and the median number of chemotherapy lines before allo-HSCT was 4 (range, 2–6). Sixteen patients (30.8%) had previously undergone auto-HSCT, and the median time from diagnosis and auto-HSCT to allo-HSCT was 27.1 months (range, 6.2–117.7 months) and 18.5 months (range, 6.5–44.8 months), respectively. The disease status at the time of transplantation was CR (n = 14, 26.9%), PR (n = 16, 30.8%), and active disease (n = 22, 42.3%). Donor types included matched sibling (n = 18, 34.6%), haploidentical (n = 18, 34.6%), matched unrelated (n = 11, 21.2%), and unrelated donors with one allele mismatch (n = 5, 9.6%). The conditioning regimen comprised MAC (n = 2, 3.9%) and RIC (n = 50, 96.1%). Half of the enrolled patients were ABO-type matched (n = 26, 50.0%), 27 (51.9%) were in donor-to-recipient sex mismatch, and 44 (84.6%) were both donor and recipient cytomegalovirus (CMV) IgG seropositive. Table 2 presents the demographic information of the patients who underwent allo-HSCT.
Response rate, survival outcomes, and complications
Over a median follow-up period of 38.3 months (range, 1.9–112.0), the estimated 5-year OS and EFS were 38.4% (95% CI, 24.7–51.8) and 30.6% (95% CI, 18.8–43.3), respectively. The estimated 5-year CIR, NRM, and GRFS were 36.7% (95% CI, 23.6–49.8), 32.7% (95% CI, 20.3–45.6), and 15.1% (95% CI, 6.9–26.2), respectively. Figure 1 shows the 1-year (100 days outcomes in CIR and NRM) and 5-year survival outcomes. Compared to the active-disease group, the remission-achieved group showed a significantly superior rate of CR in the first 3 months after allo-HSCT (76.7% vs. 36.4%, p = 0.003) and at the last follow-up (50.0% vs. 13.6%, p = 0.006) (Fig. 2). Moreover, except for NRM (26.7% vs. 40.9%, p = 0.217), the clinical outcomes of OS (54.1% vs. 15.6%, p = 0.001), EFS (46.4% vs. 9.1%, p < 0.001), and GRFS (22.9% vs. 4.6%, p = 0.002) were significantly superior in the remission-achieved group with lower CIR (26.9% vs. 50.0%, p = 0.047). In detail (Fig. 3), among patients in the remission-achieved group before allo-HSCT (n = 30), 23 achieved CR, one achieved PR, four experienced disease relapse after allo-HSCT and died due to disease progression, and three died after engraftment (two from bacterial septic shock and one from veno-occlusive disease [VOD]) without relapse. In contrast, among patients in the active-disease group before allo-HSCT (n = 22), eight achieved CR. However, only two remained in CR, four experienced disease relapse, and two died due to septic shock during disease remission. All eight of the remaining patients who achieved PR eventually relapsed, and six died after engraftment either due to allo-HSCT-related complications (one with grade IV hemorrhagic cystitis combined with renal failure, one with VOD, and two with grade IV acute hepatic GVHD complicated with liver failure) or infection (two with CMV pneumonia).
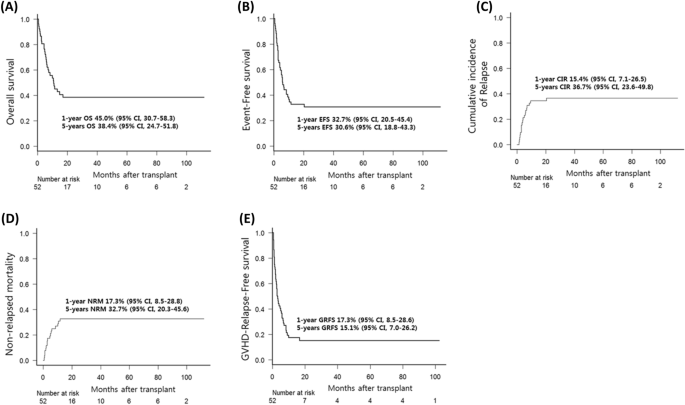
Survival outcomes of patients with relapsed/refractory diffuse large B-cell lymphoma after undergoing allogeneic hematopoietic stem-cell transplantation. The estimated 1- and 5-year (A) OS is 45.0% (95% CI, 30.7–58.3) and 38.4% (95% CI, 24.7–51.8). The estimated 1- and 5-year (B) EFS is 32.7% (95% CI, 20.5–45.4%) and 30.6% (95% CI, 18.8–43.3). The CIR and NRM at day 100 after allo-HSCT is (C) 15.4% (95% CI, 7.1–26.5) and (D) 17.3% (95% CI, 8.5–28.8). Furthermore, the estimated 5-year CIR and NRM are 36.7% (95% CI, 23.6–49.8) and 32.7% (95% CI, 20.3–45.6), respectively. The estimated 1- and 5-year (E) GRFS is 17.3% (95% CI, 8.5–28.6) and 15.1% (95% CI, 7.0–26.2). CI, confidence interval; CIR, cumulative incidence of relapse; EFS, event-free survival; GRFS, graft-versus-host disease-free, relapse-free survival; HSCT, hematopoietic stem-cell transplantation; NRM, non-relapsed mortality; OS, overall survival; R/R DLBCL, relapsed/refractory diffuse large B-cell lymphoma.
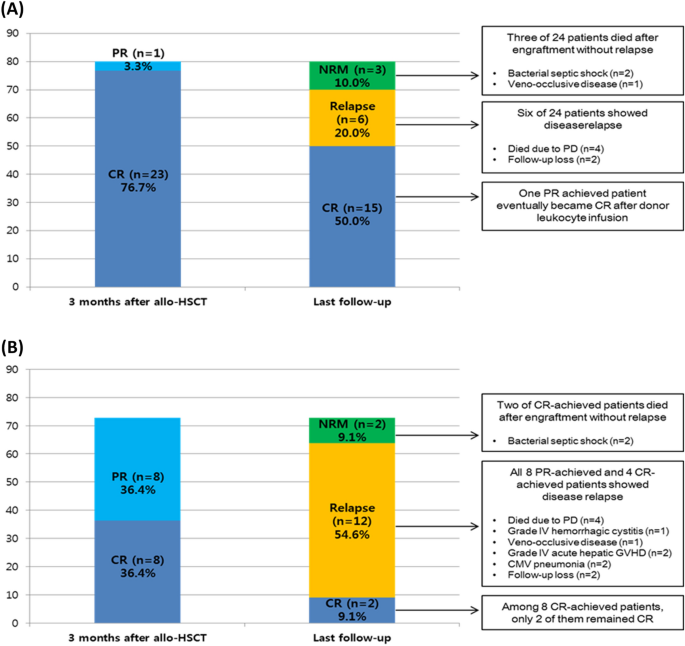
Response rate and clinical course of patients with diffuse relapsed/refractory large B-cell lymphoma after undergoing allogenic hematopoietic stem-cell transplantation. (A) Remission-achieved group: Among 30 patients in the remission-achieved group, the overall response rate (23 CR and 1 PR) was 80.0% (n = 24) at 3 months after allo-HSCT. At the last follow-up, 15 patients remained CR (including 1 PR patient who achieved CR after donor leukocyte infusion), but three died after engraftment without relapse, and six experienced DLBCL relapse. (B) Active-disease group: Among 22 active-disease group patients, the overall response rate (8 CR and 8 PR) was 72.7% (n = 16) at 3 months after allo-HSCT. However, at the last follow-up, only two patients remained CR, two died after engraftment without relapse, and 12 (4 CR and 6 PR) experienced DLBCL relapse. CMV, cytomegalovirus; CR, complete remission; GVHD, graft-versus-host disease; HSCT, hematopoietic stem-cell transplantation; NRM, non-relapsed mortality; PD, progression of disease; PR, partial remission.
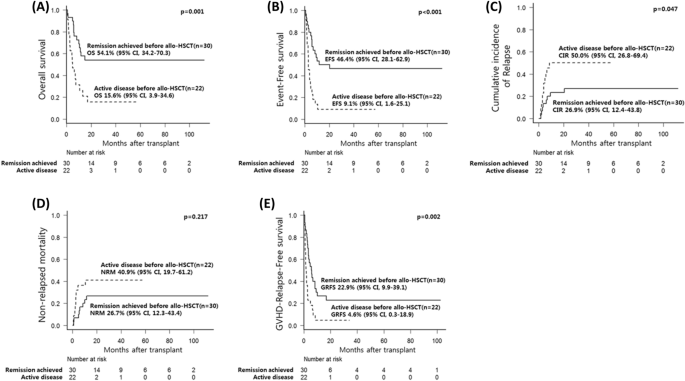
Comparison of survival outcomes between the remission-achieved and active-disease groups in patients with diffuse large B-cell lymphoma who underwent allogeneic hematopoietic stem-cell transplantation. The clinical outcomes of (A) OS (54.1% vs. 15.6%, p = 0.001), (B) EFS (46.4% vs. 9.1%, p < 0.001), and (E) GRFS (22.9% vs. 4.6%, p = 0.002) were significantly superior in the remission-achieved group with (C) lower CIR (26.9% vs. 50.0%, p = 0.047), except for (D) NRM (26.7% vs. 40.9%, p = 0.217). CI, confidence interval; CIR, cumulative incidence of relapse; EFS, event-free survival; GRFS, graft-versus-host disease-free, relapse-free survival; HSCT, hematopoietic stem-cell transplantation; NRM, non-relapsed mortality; OS, overall survival; R/R DLBCL, relapsed/refractory diffuse large B-cell lymphoma.
The overall cumulative incidence of grade 3 to 4 acute GVHD and moderate-to-severe chronic GVHD that required steroid pulse therapy was 17.3% (95% CI, 8.5–28.8%) and 29.1% (95% CI, 17.2–42.0%), respectively. The active-disease group had a significantly higher incidence of grade 3–4 acute GVHD than the remission-achieved group before allo-HSCT (6.7% vs. 31.8%, p = 0.023). However, no significant differences in moderate-to-severe chronic GVHD incidence (37.1% vs. 18.2%, p = 0.172) were observed between the two groups. The allo-HSCT-related complication incidence, response rate, and survival outcomes in the remission-achieved and active-disease groups before allo-HSCT are presented in Table 3.
Prognostic factor analysis
The results of the univariate analysis for OS, EFS, CIR, NRM, and GFRS are presented in Supplementary Tables 1 and 2. In the multivariate analysis, a shorter interval from diagnosis to allo-HSCT (median of < 27.1 months), which reflects relatively rapid disease progression, showed significantly poor OS (hazard ratio [HR], 3.92; 95% CI, 1.83–8.43; p < 0.001) and EFS (HR, 2.65; 95% CI, 1.28–5.46; p = 0.008). Complex karyotypes in BM involving DLBCL were also associated with poor OS (HR, 1.42; 95% CI, 1.06–1.90; p = 0.018) and NRM (HR, 1.41; 95% CI, 1.02–1.94; p = 0.040). Active disease before allo-HSCT was associated with significantly lower EFS (HR. 2.50; 95% CI, 1.21–5.17; p = 0.014), GFRS (HR, 2.54; 95% CI, 1.37–4.72; p = 0.003), and higher CIR (HR, 3.03; 95% CI, 1.14–8.02; p = 0.026). The MAC regimen for allo-HSCT was associated with significantly higher CIR (HR, 11.3; 95% CI, 3.33–38.1; p < 0.001), and patients with previous autologous stem-cell transplantation (ASCT) had significantly better GRFS (HR, 0.50; 95% CI, 0.26–0.98; p = 0.043). The results of the multivariate analysis are presented in Fig. 4.
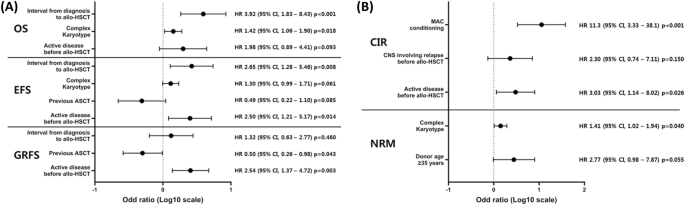
Multivariable analysis of survival outcomes related to allogeneic hematopoietic stem-cell transplantation in patients with relapsed/refractory diffuse large B-cell lymphoma. (A) The multivariable analysis for each survival outcome shows that a shorter interval of the median of < 27.1 months from diagnosis to allo-HSCT (HR, 3.92; 95% CI, 1.83–8.43; p < 0.001) and complex karyotype presenting bone marrow (HR, 1.42; 95% CI, 1.06–1.90; p = 0.018) are significantly related to poor OS. In the case of EFS, a shorter interval compared to the median of < 27.1 months from diagnosis to allo-HSCT (HR, 2.65; 95% CI, 1.28–5.46; p = 0.008) and active disease before allo-HSCT (HR, 2.50; 95% CI, 1.21–5.17; p = 0.014) are significantly related to poor EFS. Previous ASCT are significantly related to better GRFS (HR, 0.50; 95% CI, 0.26–0.98; p = 0.043), but active disease before allo-HSCT are significantly related to poor GRFS (HR, 2.54; 95% CI, 1.37–4.72; p = 0.003). (B) Active disease before allo-HSCT (HR, 3.03; 95% CI, 1.14–8.02; p = 0.026) is also significantly related to higher CIR with MAC conditioning (HR, 11.3; 95% CI, 3.33–38.1; p < 0.01). Complex karyotype presenting bone marrow is also related to higher NRM (HR, 1.41; 95% CI, 1.02–1.94; p = 0.040). CI, confidence interval; ASCT, autologous stem-cell transplantation; CIR, cumulative incidence of relapse; EFS, event-free survival; GRFS, graft-versus-host disease free, relapse-free survival; HR, hazard ratio; HSCT, hematopoietic stem-cell transplantation; MAC, myeloablative conditioning; NRM, non-relapsed mortality; OS, overall survival; R/R DLBCL, relapsed/refractory diffuse large B-cell lymphoma.
- SEO Powered Content & PR Distribution. Get Amplified Today.
- PlatoData.Network Vertical Generative Ai. Empower Yourself. Access Here.
- PlatoAiStream. Web3 Intelligence. Knowledge Amplified. Access Here.
- PlatoESG. Carbon, CleanTech, Energy, Environment, Solar, Waste Management. Access Here.
- PlatoHealth. Biotech and Clinical Trials Intelligence. Access Here.
- Source: https://www.nature.com/articles/s41598-023-44241-0