Multiple nucleation biomineralization to prepare the SIOM entirely composed of HAP
We used the natural biomineralization strategy for tooth enamel to prepare the SIOM, which fully composed of HAP20. Tooth enamel is comprised of dense HAP biomineralized via controlled ion adsorption (Fig. 2a)21,22. In particular, the osteopontin (OPN) favorably interacts with PO43- ion, while dentin matrix acidic phosphoprotein 1 (DMP1) captures Ca2+ 23,24. These selective ion adsorptions enable a characteristic enamel growth, i.e., multiple nucleation biomineralization for dense coverage of HAP. Accordingly, we developed a selective ion-adsorbing zwitterionic layer in the CM. (Fig. 2b). This zwitterionic membrane (ZM) was fabricated by conducting dual radical-based zwitterionic sulfobetaine polymerization on the CM (Supplementary Fig. 1a)25. The significant zwitteration of the CM was confirmed using X-ray photoelectron spectroscopy, ion mapping, and time-of-flight secondary ion mass spectrometry (Supplementary Fig. 1b–e). The zwitterionic groups functioned as nucleation sites, similar to OPN and DMP1. Specifically, the positive moiety of the ZM (–N+R4–) preferentially interacted with the PO43− ions, and the negative moiety (–SO3−–) was bound to Ca2+. These selective ion adsorptions determined the biomineralization kinetics, as shown in Supplementary Fig. 2. Thus, the ZM enabled the multiple nucleation biomineralization and full coverage of HAP within the SIOM, as will be discussed in the following sections26.
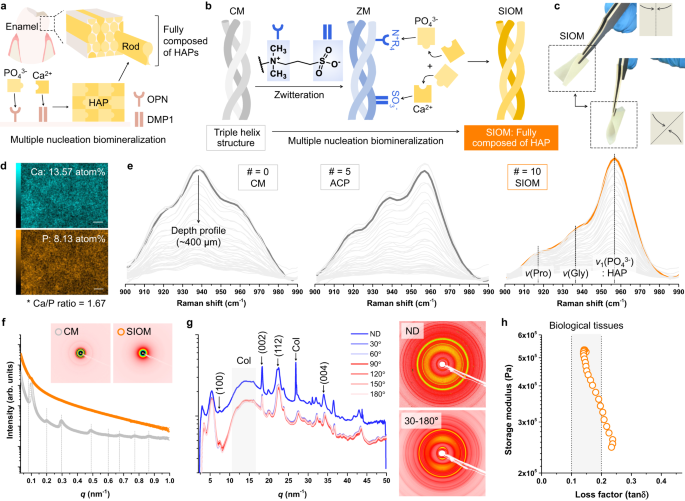
a Natural multiple nucleation biomineralization process for constructing dense tooth enamel structures. b Schemes depicting the osteo-mimetic zwitteration of the CM into a zwitterionic membrane (ZM) and the multiple nucleation biomineralization process emulated to obtain an entirely biomineralized SIOM. c Representative photographs of the SIOM (1 × 1 cm2). d Ca and P ion mapping of the SIOM acquired using an energy-dispersive spectrometer. Scale bar = 2 μm. e Raman spectra at 900–990 cm−1. The light gray lines indicate the depth profiles measured per 10 μm up to 400 μm. The black and orange bold lines indicate the top surface results. ACP represents amorphous calcium phosphate. f One-dimensional and two-dimensional small-angle X-ray scattering (SAXS) patterns of the CM and SIOM. q is the scattering vector, where q = (4π/λ) sin(θ/2). θ and λ are the scattering angle and wavelength of the incident X-ray beam, respectively. g One-dimensional and two-dimensional wide-angle X-ray scattering (WAXS) patterns of the SIOM. X-rays were irradiated in the normal direction (ND; z axis) and cross-sectional direction (x–y axis) of the SIOM. h Storage modulus vs. loss factor (tanδ) plot of SIOM. Source data are provided as a Source Data file.
The ZM was repeatedly exposed to 0.3 M PO43− and 0.5 M Ca2+ to advance its biomineralization into the SIOM27. Fig. 2c shows the image of the prepared 1 × 1 cm2 SIOM. The SIOM was tractable and could be readily used for GBR (Supplementary Fig. 3). The SIOM had a Ca/P ratio of 1.67, indicating that thermodynamically stable HAP [Ca10(PO4)6(OH)2] was generated (Fig. 2d). In particular, the SIOM was obtained after undergoing ion exposure 10 times (#= 10, where # is the number of PO43−–Ca2+ exposure sets). The entire depth Raman profiles were monitored by increasing # from 0 (CM) to 10 (SIOM) (Fig. 2e). The CM exhibited apparent Raman signals of proline and glycine at ~920 cm−1 and ~935 cm−1, respectively. The HAP signal at ~955 cm−1 intensified when # was 5, implying that amorphous calcium phosphate was generated26. When # reached 10, the HAP signal of the SIOM intensified significantly. The X-ray diffraction spectrum of the SIOM displays the characteristic HAP pattern (Supplementary Fig. 4).
Subsequently, the CM and SIOM were investigated using SAXS (Fig. 2f). The SAXS pattern revealed that the CM had a lamellar structure with a d-spacing of 63 nm28. However, this lamellar structure disappeared after the CM biomineralized into a SIOM. WAXS experiments were conducted, as shown in Fig. 2g. X-rays were transmitted to the SIOM in the normal direction. Thereafter, cross-sectional WAXS signals were obtained by rotating the X-ray by 30° at the x–y plane of the SIOM. Regardless of the X-ray incidence angle, the SIOM exhibited distinct HAP peaks, namely, (002), at 18.3 nm−1. The mercury intrusion porosimeter experiments suggested that the SIOM featured a denser submicron pore structure than CM (Supplementary Fig. 5). Accordingly, we concluded that the entire CM was completely biomineralized into a SIOM. Moreover, the fully covered HAP compensated for the free radical-induced decreased mechanical property of the ZM (Supplementary Fig. 6). In other words, the application of SIOM means an establishment of a durable and tooth enamel-like ordered structural environment during GBR therapy.
When a developed material is applied to a specific tissue, it should exhibit similar viscoelasticity to surrounding tissues for a satisfactory operation29. The viscoelasticity of SIOM was studied through the storage modulus vs. loss factor profile (Fig. 2h)30,31. The loss factors of most biological materials involving extracellular matrix, soft tissues, and hard tissues are in the range of 0.1–0.232. Remarkably, the viscoelasticity of the SIOM was comparable to the biological tissues. Therefore, SIOM is physically beneficial when deployed at the interface of the gingival gum and the alveolar bone defect.
Structural stability of the SIOM under enzymatic degradation conditions
During several months of GBR therapy, the occlusive membrane should maintain its structure to provide sufficient time and space for alveolar bone regeneration. In the early phase of regenerative healing, catabolic enzymes and primary response inflammatory cytokines are generated, which affects the stability of the occlusive membrane33,34. Although collagenase type I is a necessary regeneration-associated enzyme, it causes the rapid degradation of CMs, collapsing the closed healing zone. Accordingly, the enhanced enzymatic stability of SIOM should be established. Moreover, we functionalized the CM with various charge groups (R) to evaluate the significance of osteo-mimetic multiple nucleation biomineralization in yielding outstanding stability (Fig. 3a). Negative membrane (NM) and positive membrane (PM) were prepared with two strong polyelectrolytes: polystyrene sulfonate and poly(diallydimethylammonium chloride). ZM-1 is a sulfobetaine zwitterionic polymer, the original component of the SIOM. ZM-2 is a phosphorylcholine zwitterionic polymer. Subsequently, the NM, PM, ZM-1, and ZM-2 were biomineralized in the same manner as the SIOM, i.e., # = 10 with 0.3 M PO43− and 0.5 M Ca2+. The NM and PM possessed a single nucleation site. Therefore, HAPs were grown into spherically aggregated structures via single nucleation biomineralization (Fig. 3b)35. Owing to the sparsely distributed granular HAPs, the collagen substrate was still visible on the biomineralized NM and PM surfaces. In contrast, ZM-1 and ZM-2 underwent multiple nucleation biomineralization, producing fully covered wrinkled flake HAPs. In summary, osteo-mimetic multiple nucleation biomineralization is essential for the full coverage of HAPs within SIOM.
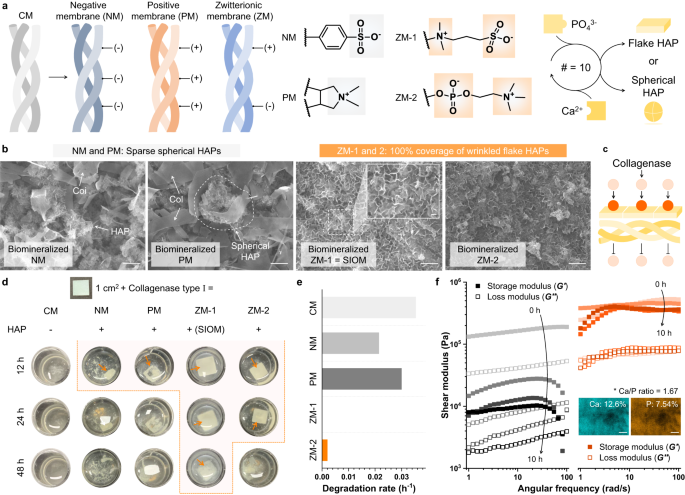
a Functionalization of the CM with different charge groups. The chemical structures of a negative membrane (NM), a positive membrane (PM), and two ZMs are suggested. The characteristics of the substrate determine the HAP geometry. b Scanning electron microscope images of the biomineralized NM, PM, and ZM-1. Scale bar = 1 μm. n = 5 images per membrane group. c Schemes of collagenase penetration through the biomineralized NM, PM, and ZM. d Images of the CM and the biomineralized NM, PM, ZM-1, and ZM-2 after being immersed in collagenase media (0.2 IU mL−1). The orange arrows indicate the residual membranes. e Degradation rates of the CM and the biomineralized NM, PM, ZM-1, and ZM-2. f Rheological responses of the CM (left) and SIOM (right) during 10 h of enzymatic degradation. The inserted ion mapping image was obtained from the SIOM after the end-point of collagenase exposure. Scale bar = 2 μm. Source data are provided as a Source Data file.
The densely grown HAPs physically and electrostatically blocked collagenase penetration, thereby improving the enzymatic stability of the SIOM (Fig. 3c). To prove this concept, the pristine CM and the biomineralized NM, PM, ZM-1, and ZM-2 were immersed in collagenase type I media and incubated at 37 °C (Fig. 3d)36. The CM degraded rapidly within 12 h, demonstrating its practical limitation with spacing durability. Meanwhile, the CM exhibited excellent stability for hydrolytic degradation (Supplementary Fig. 7). As shown in Fig. 3e, the degradation rate (h−1) was determined by assessing the residual membrane within 12 h. The biomineralized NM and PM presented slightly decreased degradation rates: 0.035 h−1 of CM, 0.025 h−1 of NM, and 0.029 h−1 of PM. However, they degraded after 12 h of enzyme exposure since the sparsely distributed HAPs could partially block collagenase penetration. Meanwhile, ZM-1 and ZM-2 with fully covered wrinkled flake HAPs did not degrade within 24 h, resulting in a degradation rate <0.005 h−1. Interestingly, the residual biomineralized ZM-1 (i.e., SIOM) was monitored even after 48 h of degradation. When the CM and SIOM were immersed in an α-amylase solution, a remarkable improvement in their enzymatic stability was also observed (Supplementary Fig. 8). Moreover, the storage and loss moduli of the CM and SIOM were measured during 10 h of degradation (Fig. 3f). The CM lost ~90% of its storage modulus after 4 h of degradation, implying that the GBR zone dented rapidly. On the other hand, the SIOM maintained its original properties (e.g., shear modulus and Ca/P ratio of 1.67) even after 10 h of degradation. Accordingly, the SIOM exhibited outstanding enzymatic stability and long-lasting space formation properties.
Symbiosis-inducing effect of the SIOM
The SIOM was subjected to Good Laboratory Practice-ensured cytocompatibility tests (ISO 10993-5: 2009). Slight grade 1 reactivity was observed within a non-discernible zone, confirming the highly biocompatible performance of the SIOM (Supplementary Table 1–2). Progenitor cells, namely, BMSCs, were used to evaluate the osteoconductivity of the SIOM to confirm its cellular symbiosis-inducing performance. BMSCs and CM or SIOM were cultured in growth media and osteogenic differentiation media for 2 weeks. Subsequently, a quantitative real-time polymerase chain reaction was performed to study the expression degree of osteogenic biomarkers. Interestingly, OPN expression increased 2.67-fold in BMSCs cultured in the growth media with the SIOM, thereby indicating the increased density of osteogenic differentiation (Fig. 4a). According to BMSC tests conducted under differentiation media conditions, the SIOM exhibited significantly enhanced expression of differentiation markers: a 127% increase in RUNX2, a 118% increase in OCN, a 1065% increase in OPN, and a 2884% increase in BMP2 (Fig. 4b). The above biomarker results indicate that the osteo-mimetic SIOM mediated an excellent stimulation for osteo-differentiation37. In particular, the significantly enhanced expressions of OPN and BMP2 implied that SIOM promotes bone healing up to the bone tissue formation stage during 2 weeks. Therefore, SIOM is desirable for the GBR therapy of several months requiring the expeditious augmentation of the alveolar bone.
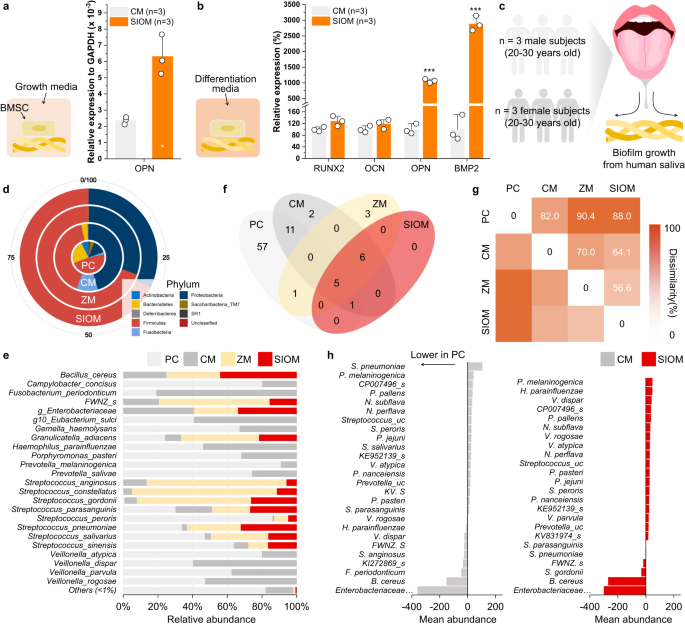
Analysis of biological responses from human bone marrow stem cells (BMSCs) via cytokine expression (RUNX2, OCN, OPN, and BMP2). BMSCs were cultured in the a growth media (mean ± SD, n = 3, two-tailed t-tests, p = 0.0317) and b osteogenic differentiation media (mean ± SD, n = 3, two-tailed t-tests, p = 0.000012 for OPN, p = 0.000249 for BMP2). c In vitro experiment protocol showing the collection of healthy human adult saliva for culture over the occlusive membranes for a 16 S RNA sequencing assay. Positive control (PC) means the group without an occlusive membrane. d Taxonomic composition for the CM, ZM, and SIOM at the phylum level in comparison to pooled saliva culture sequences. e Comparison of species level relative abundance for taxa exhibiting the highest prevalence. Taxa representing less than 1% of total sequences were grouped as others. f Core microbiota Venn plot presenting species level shared and unique taxa by overlapping regions. g The dissimilarity percentage between the groups against the pooled saliva reference computed using SIMPER analysis. h The differences in abundances of taxonomic groups with greater than 1% contribution to dissimilarity to PC. The negative values in x axis indicate lower abundance in PC compared to CM/SIOM and vice-versa. RUNX2: runt-related transcription factor 2; OCN osteocalcin, OPN osteopontin, BMP2 bone morphogenic protein-2. Source data are provided as a Source Data file. *p < 0.05, **p < 0.01, ***p < 0.001.
The nature of the microbiota-contacting substrate closely determines the microbial ecology in the vicinity38. Here, the symbiosis-inducing effect of the SIOM was investigated by monitoring whether a healthy microbiome community was constructed at the SIOM. To study the microbiome development at the SIOM, we used 16 S rRNA sequencing of co-cultured salivary extracts from six healthy adults (Fig. 4c). The observed operational taxonomic units in the sequencing showed a distinct early plateauing curve for the ZM and SIOM with low sequencing, indicating a genuine lack of diversity (Supplementary Fig. 9)39. As shown in Fig. 4d, the Firmicutes-to-Bacteroidetes (F/B) ratio increased significantly (ca. 49.0-fold) during the microbial community level interaction at the ZM and SIOM. Specifically, the gram-negative classes of Bacteroidetes reduced remarkably (Supplementary Fig. 10). This F/B profile is associated with competition for the metabolic fermentation pathway and interacts negatively in the human gut40. Moreover, a low F/B gut profile has been co-associated with increased pro-inflammatory cytokine expression41,42. Thus, a settled microbiome community with an unilaterally low F/B scan may impede normal healing through a chronic expression of pro-inflammatory cytokines.
As shown in the relative abundance at genus level (Supplementary Fig. 11), three periodontal pathobionts serving as taxonomic biomarkers, namely, Prevotella, Allopreveotella, and Actinomyces, did not exhibit any abundance at SIOM43,44. More specific observations could also be made on resolving the differences at the species level resolution (Fig. 4e). The species with pathobiont nature, Fusobacterim periodonticum, Gemella haemolysans, Haemophilus parainfluenzae, Porphyromonas pasteri and Veillonella sps groups, remained undetected from the SIOM (Supplementary Fig. 12). Furthermore, SIOM exhibited a lower abundance of the bridging species, Veillonella, which leads to dysbiosis by acting as an accessory pathogen for keystone pathobionts45,46. In particular, Veillonella parvula, Veillonella dispar, and Veillonella rogosae were found in higher concentrations in CM. This result is associated with the actual lack of gamma diversity as the Hill number increased (Supplementary Fig. 13)39. Typically, a shifted microbiome is described as a niche-specific species turnover (gain or loss). Accordingly, the near total lack of pathobionts (especially Bacteroidetes and Actinobacteria) indicates that the microbiome community at the SIOM prefers commensal oral microbionts47.
Typically, the core microbiota is indicative of disease–disease relationship and it is varied by immediate environmental changes48. The SIOM had a high co-occurrence representation of genera with PC, proving its potential for recovering microbial communities (Fig. 4f). In contrast, the ZM formed unique taxa and core microbiota distribution: Bacteroides vulgatus, Enterococcus faecium groups, and Romboutsia timonensis (Supplementary Data 1). In this context, the ZM was insufficient to induce a healthy microbiome although its zwitterionic groups nonspecifically prevented microbial growth up to 50% (Supplementary Fig. 14)49. Hence, ZMs without osteo-mimetic multiple nucleation biomineralization may be the tipping point for disturbed microbiomes50.
We also observed that the SIOM significantly impacted the overall diversity similarity index (Fig. 4g). The ZM and SIOM showed a high dissimilarity (>79%) to the PC reference. Most of the observed differences could be attributed to the variations in the core microbiota (>70% prevalence)51. Fig. 4h draws the comparison with the incubate of native pooled salivary microbiota (PC), and Supplementary Fig. 15 shows the entire name of taxonomic groups. Regarding both CM and SIOM, the dissimilarity contribution was observed to be highest for Enterobacteriaceae and Bacillus cereus groups. However, V.dispar, P. melaninogenica, and F. periodonticum had ~3% dissimilarity contribution with higher abundance expressed at the CM interface. Furthermore, in specific periodontally related indicator species (Supplementary Note), the pathogenic Porphyromonas and Fusobacterium genera were observed in the PC and CM groups only.
However, due to the sampling of saliva from a healthy cohort, it was limited in identifying the keystone species for periodontal pathogenesis using amplicon sequencing. Accordingly, we conducted Porphyromonas gingivalis and Staphylococcus aureus colony forming experiments to assess the specific microbial interaction (Supplementary Fig. 16). Remarkably, SIOM showed a 68% decreased P. gingivalis colony compared to the CM. Moreover, SIOM exhibited a 54% reduction in S. aureus colony formation. In particular, S.aureus is one of the pathogens with a favorable affinity towards titanium implants and found in the early microbiota after surgery52. Considering that SIOM deployed near dental implants, its strong resistance against P. gingivalis and S. aureus further confirms its enhanced performance for satisfactory GBR outcome. Supplementary Fig. 17 shows the unsupervised pattern analysis with the Spar CC method. Notably, the species positively correlated to the identified pathobionts (P. pasteri, F. nuceatum, and F. periodonticum) had low relative abundance in SIOM. In other words, the SIOM exhibited a weaker correlation with the pathobionts. In conclusion, we confirm that the SIOM had an improved symbiosis-inducing effect based on its favorable cellular and prokaryotic response.
In vivo canine open healing GBR study
We studied GBR therapy to verify that the SIOM induced a symbiotic regeneration environment in a complex and challenging cases. As shown in Fig. 5a, the open healing of the SIOM-assisted GBR process was investigated in a medium-sized canine model. This canine premolar model offers excellent anatomical similarity to the human alveolar region. During the healing periods, the CM or SIOM was exposed to the oral cavity and came into contact with saliva and gingival crevicular fluid (GCF)53. A balanced and diverse oral environment, i.e., symbiosis, promotes physiological healing, while the absence of symbiosis precipitates an environment that interrupts the healing process54. This scenario is critical in the early stages when the bacterial interactions feature a more significant impact. Hence, within 48 h of post-GBR surgery, we obtained microbiome information from the supra-membranous region and monitored the surgical wound closure percentage (Fig. 5b)34. Fig. 5c describes the sample gathering period, with the GBR surgery point (Sx) serving as the standard. Additionally, GCF was collected from pristine gingival crevices as a healthy symbiosis reference 24 h before GBR surgery (Sx-24). The free gingival tissue (Gingiva) and the sub-apically inflamed granular tissue (Inflamed; pathogenic reference) were acquired at Sx. These GCF, Gingiva, and Inflamed samples were further subjected to microbiome analysis. The multinomial logistic-normal model revealed no significant effect of time on microbial variance.
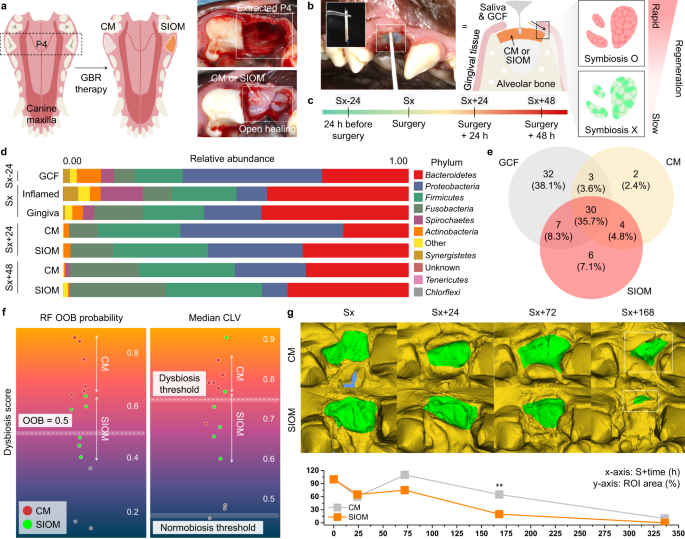
a Illustration of the split-mouth experiment protocol. The third premolar (P4) of a mongrel (medium-sized dog) was hemi-sectioned and extracted. The CM and SIOM were placed to cover the defect and secured with eight sutures. b, c Periodic sampling protocol and timeline. The sterile paper was used to acquire the microbiome samples. The gingival crevicular fluid (GCF) and saliva dynamically interacted with the CM and SIOM as the peripheral gingival tissues underwent healing. d Taxonomic relative abundance at the phylum level presented across the sampling timeline. e Core microbiota distribution between the GCF, CM, and SIOM, observed at the species level resolution. f Dysbiosis scores presented using out-of-bag (OOB) probability scores and median community-level variations (CLVs). The dysbiosis threshold was established with pre-surgical GCF samples on a scale of 0 to 1, where 1 indicates the maximum dysbiosis score. g Healing rate of the post-surgical wound (n = 7, RM ANOVA, p = 0.002) compared by identifying the region of interest (ROI; y-axis) and its reduction with time (x-axis). Source data are provided as a Source Data file. *p < 0.05, **p < 0.01, ***p < 0.001.
Based on posterior prior analysis, differential ranking analysis was performed to compare the microbiome information for each group55. In particular, comparisons were made between the baseline GCF samples and the CM and SIOM. Initially, the GCF showed a grouping pattern for species richness against sequence sample size. Contrarily, the SIOM showed a change in species richness, becoming more distinct at Sx+48 (Supplementary Fig. 18). The alpha diversity metric at the sequence level evidenced a reduction in diversity for the SIOM compared to the CM, implying fewer unique operational taxonomic units in the SIOM (Supplementary Fig. 19). ANCOM-BC analysis suggested that both the CM and SIOM showed differentially abundant phylum-level expression when compared to the GCF (Supplementary Fig. 20). The beta-coefficient magnitude and its direction in Supplementary Table 3 indicate the degree of differential abundance with larger absolute values representing stronger differential abundance.
Although CM and SIOM exhibited an increase in the relative abundance of the Fusobacteria content, SIOM presented a resistance towards Proteobacteria expression, with a progressive reduction up to the Sx+48 point (Fig. 5d). An increase of Proteobacteria expression in lesions has been observed when progressing to periodontitis in dogs56. Accordingly, the monitored progressive reduction in the SIOM means its differential resistance to Proteobacteria. Furthermore, the SIOM featured an improved expression of the core and other microbiota with an overall 8.3% overlap with GCF (Fig. 5e). Moreover, the overlapping species were notably higher at 10.8% when resolving the SIOM’s identified taxa at Sx+48 point (Supplementary Fig. 21). In contrast, the CM had an overall 3.6% overlap, which was particularly lower (2.2%) at the same time point. Thus, the SIOM was capable of resembling the native oral environment during the GBR therapy.
Two statistical indexes were used to quantify the symbiosis-inducing performance of the SIOM: OOB predicted probability and CLVs (Fig. 5f). OOB and CLV (neighborhood classification method by community) are scoring indexes for disturbed symbiosis, i.e., dysbiosis47. The dysbiosis threshold was defined from the GCF. The SIOM had a low to medium OOB score, whereas the CM had a predominantly high dysbiosis score (>0.6). The SIOM showed primary distribution under the dysbiosis threshold (0.74) in the median CLV score. Both results indicate that the SIOM resisted dysbiosis induction more effectively than the CM. In other words, osteo-mimetic SIOM positively promotes a microbiome community desirable for regeneration. Although the SIOM’s enhanced resistance towards dysbiosis was proved in vivo, there is a limited similarity (16.4%) of the bacterial taxa between canines and humans57. Given this limitation, it would be premature to explore a mechanistic rationale with the currently available data.
Figure 5g showed the rapid gingival tissue regeneration under the SIOM-triggered well-established microbial symbiosis. Notably, the SIOM presented a marked reduction in the early surgical wound size within Sx+72. Furthermore, it achieved near complete healing in less than one week of GBR therapy (Sx+168). At Sx+168, the SIOM and CM exhibited significant differences. When the CM was deployed, the healing efficiency of the SIOM at Sx+168 took twice as long (Sx+336) to achieve. Although HAP has outstanding physio-functions in promoting hard tissue regeneration and cellular differentiation58,59, its relevance to soft tissue regeneration is rarely reported. On the other hand, the importance of microbiota composition in the systemic regeneration process has been gradually revealed60. In this context, Fig. 5g implies that the SIOM-based symbiosis induction significantly helps an expeditious healing response during GBR therapy.
In vivo canine closed healing under the inflammatory-challenged condition
Osteo-immunogenic assays provide information on the healing progress of a complex periodontal defect. During GBR therapy, it is important to create a space that is separate from other tissues and to use an occlusive membrane to preserve that space for closed healing61. However, during healing periods, prolonged inflammation causes connective tissue hyperplasia, which deforms the occlusive membrane and compromises the healing space11. The inflammation is generally caused by bacterial metabolites, such as lipopolysaccharides, which trigger cytokine expression in neutrophils, macrophages, and B-cell immune cells62,63. Accordingly, the inflammation would limit the amount of bone formation in the closed healing zone.
In this study, an inflammatory–challenged closed healing case study further confirmed the symbiosis-inducing capacity of the SIOM in vivo. Chronic periodontal and endodontic lesions were induced for 9 weeks to prepare the inflammatory–challenged environment in soft and hard tissues, which featured severe periodontitis and peri-apical granulomatous lesions (Fig. 6a). Following infected roots extraction, bone defect was treated with synthetic bone substitute with either SIOM or CM, and subsequently covered with the inflamed gingival tissue (Fig. 6b). A contralateral socket was prepared as a comparison reference and denoted as blank. Blank group means the untreated and uninflamed region under spontaneous healing without pin fixation. The study on the closed healing model was limited to immuno-osteogenic bioactivities, and invasive sample collection for microbiome analysis was impossible.
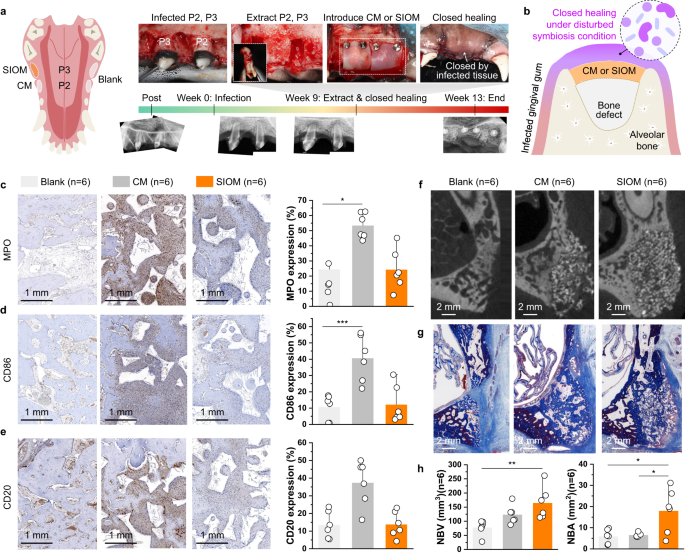
a Inflammatory-challenged defect model and the intervention protocol. The second and third maxillary premolar (P2 and P3) with ligature-induced periodontitis (9 weeks) exhibits apical granulomatous lesions. The subsequent extraction and delivery of the SIOM and CM were followed by pin fixation. A contralateral root was prepared as a blank control reference. b After-extraction defects treated with a bone substitute and the occlusive membrane (CM or SIOM), with a complete flap approximation and surgical wound closure. c–e Immuno-histological profile and corresponding stained intensity percentages of pro-inflammatory cytokines with specificity for c neutrophils (myeloperoxidase; MPO, mean ± SD, n = 6, ANOVA, p = 0.048), d M1 macrophages (CD86, mean ± SD, n = 6, ANOVA, p = 0.001), and e mature B cells (CD20, mean ± SD, n = 6). f Micro-CT images and g Masson’s trichrome stained histological photomicrographs obtained after 4 weeks of closed GBR therapy. h New bone volume (NBV, mean ± SD, n = 6, Kruskal, p = 0.004) and new bone area (NBA, mean ± SD, n = 6, ANOVA, p = 0.012 for blank vs. SIOM, p = 0.024 for CM vs. SIOM) measurements from micro-CT and histological photomicrographs, respectively. n indicates the number of biologically independent animals examined. Source data are provided as a Source Data file. *p < 0.05, **p < 0.01, ***p < 0.001.
To label inflammatory cell infiltrates, we used MPO for neutrophils and macrophages, CD86 for M1 macrophages, and CD20 for B cells (Fig. 6c–e). The immunohistochemical staining results revealed that MPO increased dramatically in the CM group. In contrast, the SIOM demonstrated strong resistance to neutrophil infiltration, indicating an early alleviation of the acute inflammatory phase (Fig. 6c). Furthermore, we observed that the SIOM group exhibited a 3.3-fold reduction in CD86+ expression when compared to the CM group. CD86+ expression is associated with a pro-inflammatory (M1 macrophage) response. Accordingly, this reduced biomarker expression suggests the occurrence of early macrophage polarization, which is an essential step in tissue healing (Fig. 6d)64,65. Moreover, the reduced M1 macrophage expression in the SIOM-treated defect indicated an improved resistance to foreign body reactions. Clinically, peri-implant and periodontal diseases have been recognized through a high B cell density, which is associated with acute exacerbation and aggressive inflammatory lesions66. Hence, the multifold reduction in CD20+ observed with SIOM further validates the decreased foreign body reaction (Fig. 6e). In summary, SIOM-assisted GBR therapy can prevent inflammatory responses from exacerbating even when the surrounding environment makes the healing region prone to inflammation.
While an initial inflammatory response is necessary for healing, an optimized immune response can lead to a smoother transition to the anabolic regenerative stage. In our study, the SIOM resulted in excellent biological integration, as evidenced by the micro-CT (Fig. 6f) and micromorphological analyses (Fig. 6g). We observed that the NBV of SIOM significantly improved when compared to that of the blank group. Additionally, the Masson’s trichrome-stained histological sections revealed that the NBA in the SIOM group significantly increased by ~67% and 64% in comparison to that in the CM and blank, respectively (Fig. 6h) groups. The entire above results on MPO, CD86, CD20, NBV, and NBA confirmed a symbiotically integrating GBR therapy driven by SIOM.
- SEO Powered Content & PR Distribution. Get Amplified Today.
- PlatoData.Network Vertical Generative Ai. Empower Yourself. Access Here.
- PlatoAiStream. Web3 Intelligence. Knowledge Amplified. Access Here.
- PlatoESG. Carbon, CleanTech, Energy, Environment, Solar, Waste Management. Access Here.
- PlatoHealth. Biotech and Clinical Trials Intelligence. Access Here.
- Source: https://www.nature.com/articles/s41467-023-43428-3